
If there’s one category of symptoms that sends parents into instant panic, it’s anything involving breathing.
A cough that sounds different.
Noisy breathing in the middle of the night.
A child who suddenly looks uncomfortable or distressed or off.
As a former ER nurse and a naturally minded mom, I’ve lived on both sides of this — the clinical side and the emotional side. I get it.
Even I still have moments where I ask, “Okay, is this fine or do we need to go in?”
Here’s what helped me: actually understanding what’s happening in those tiny airways. Once I knew how they worked and what actually supports them and helps them heal, I could tell the difference between ‘this is scary but okay’ and ‘we need to go in, now.’
I want to give you that same foundation — the knowledge I have and the tools I use — so you don’t have to worry. So you can feel prepared instead of panicked, confident in what you’re seeing, and clear on when home support is appropriate and when medical care is needed.
It’s not meant to replace your doctor. But the more we know, the better prepared we are, the calmer we can be.
This information is for educational purposes only and is not medical advice. Always consult a qualified healthcare provider for personalized guidance.
Affiliate Disclosure: This post may include affiliate links. If you purchase through one of these links, I may earn a small commission at no extra cost to you. I only ever share products I personally use, trust, or would feel comfortable recommending to my own family.
How the Respiratory System Works
Understanding respiratory illness starts with understanding the airways themselves.
Upper and Lower Airway
The respiratory system is divided into two main parts: Upper + Lower Airways
Upper Airway
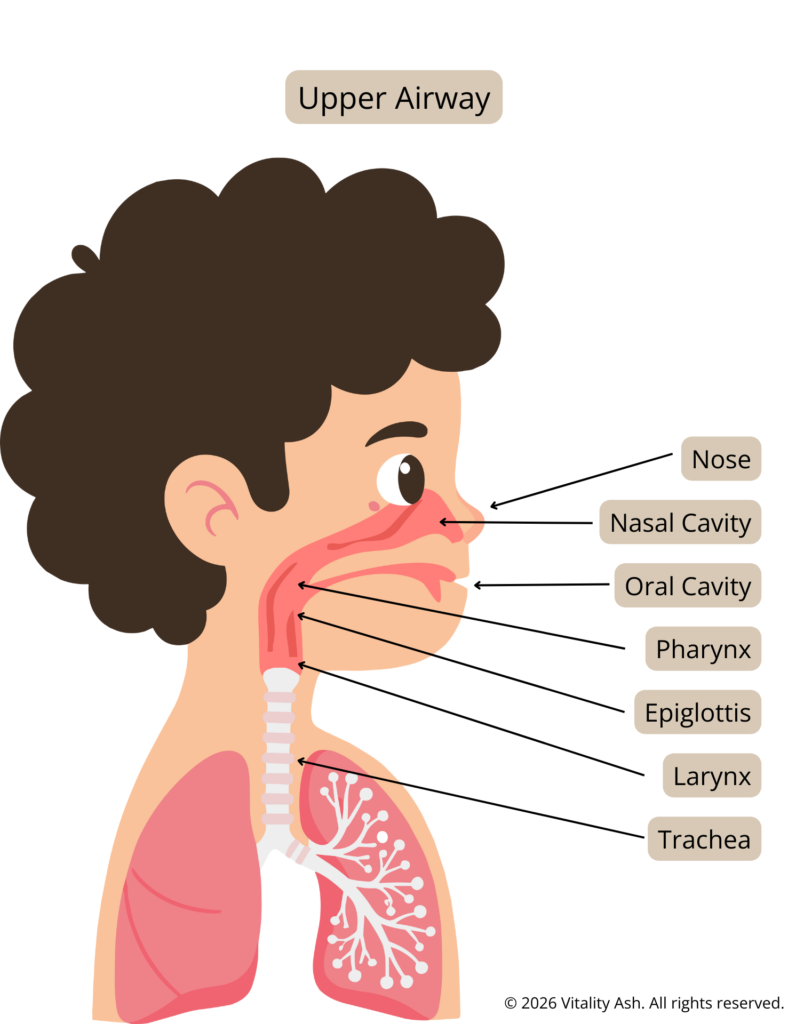
Upper Airway
- Nose
- Nasal Cavity
- Oral Cavity
- Throat (Pharynx, Epiglottis)
- Voice box (larynx)
- Trachea (windpipe)
*Note: Many childhood illnesses — especially the scary-sounding ones (like croup) — primarily affect the upper airway, not the lungs.
Lower Airway
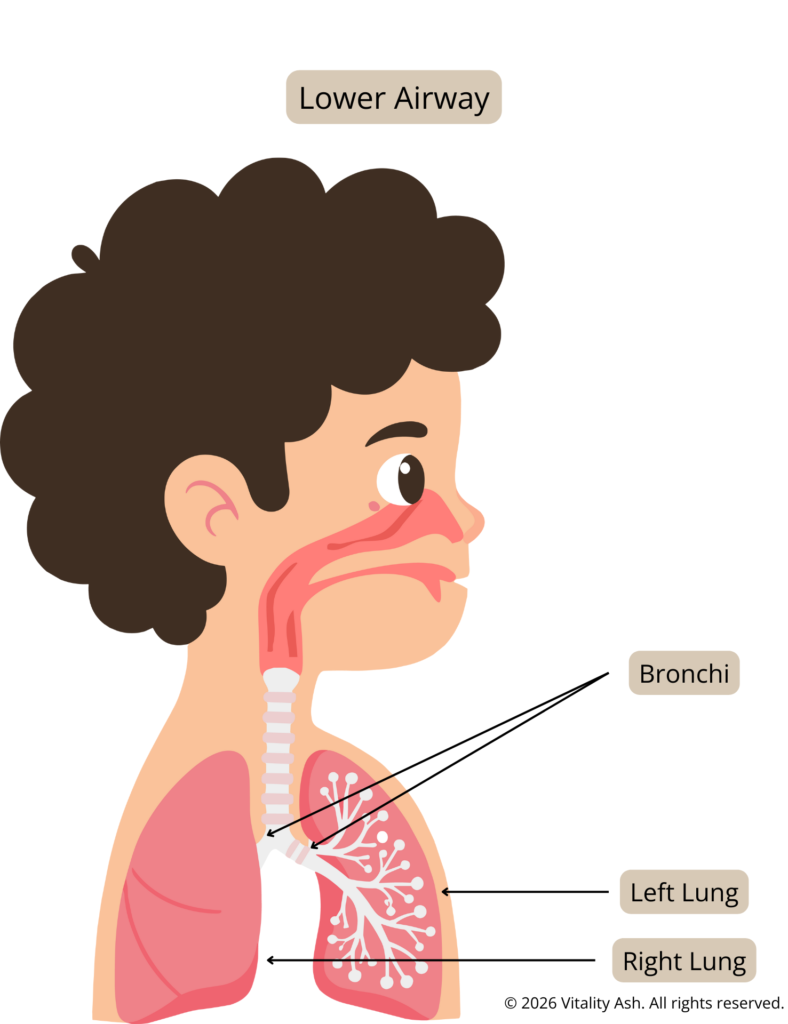
Lower Airway
- Bronchi
- Bronchioles
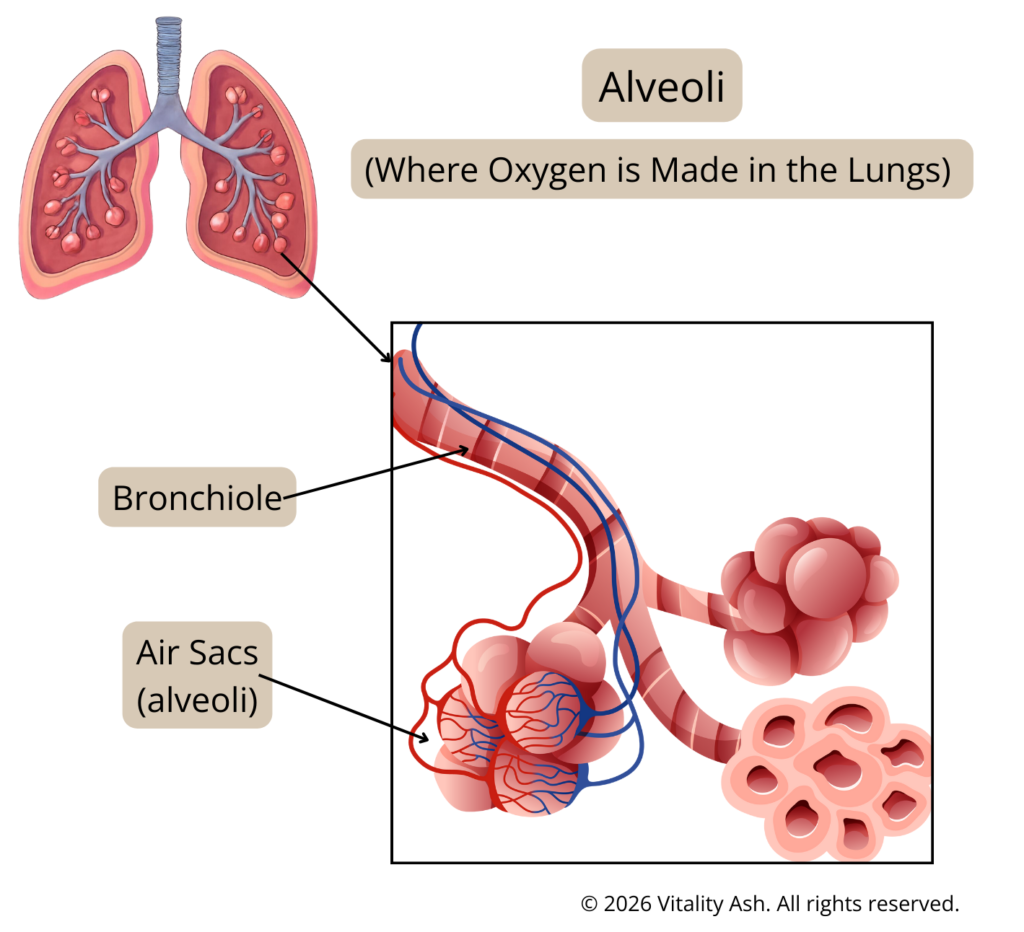
- Lungs
- Alveoli
*Note: The trachea is often classified as lower airway anatomically, but many upper airway illnesses like croup involve the trachea.
This matters because the upper airway is:
- Smaller (a smaller airway means that even a small amount of swelling can cause it to close up significantly more than an adult’s airway).
- More sensitive
- More prone to swelling
A little inflammation in a small space can sound dramatic even when oxygen levels are still okay.
The Role of Mucus, Cilia, and Humidity
The airways are lined with tiny hair-like structures called cilia. Their job is to move mucus (and trapped pathogens) upward and out.
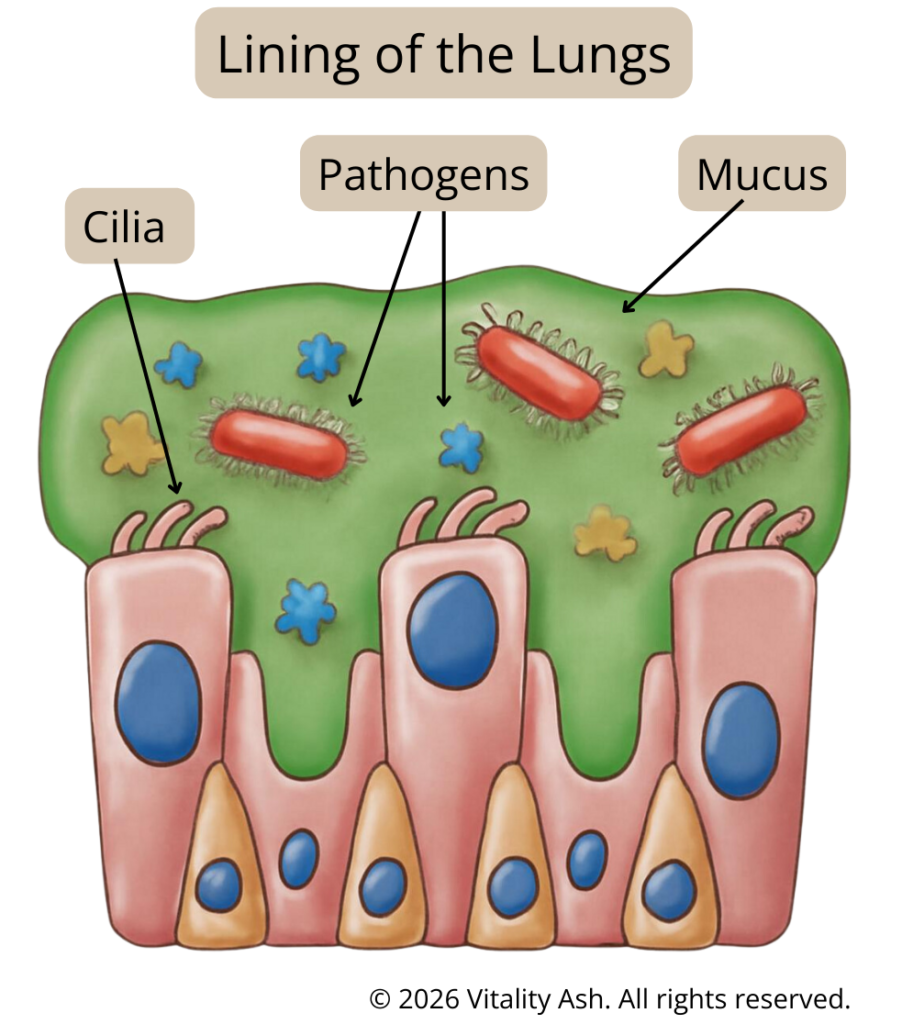
Cilia work best when:
- The air is moist
- The body is well-hydrated
- We support the body’s natural processes rather than immediately suppressing every symptom
Dry air thickens mucus and slows this process — which is why respiratory illness is often worse in winter.
Why Children’s Airways Are Different (and Why Symptoms Can Escalate Quickly)
One of the biggest reasons respiratory illness feels more alarming in babies and young children is simple:
Their physiology is different from that of adults.
Understanding these differences helps explain why symptoms can appear suddenly, why kids can tire quickly, and why monitoring matters even when things seem stable.
1. Children’s Airways Are Smaller — So Swelling Has a Bigger Impact
Another key difference between children and adults is airway size and position.
Children’s airways are:
- Narrower
- Softer
- Positioned slightly more forward than an adult’s airway
Because the airway is smaller to begin with, even mild swelling or blockage can make breathing feel harder.
Things that wouldn’t cause much trouble in an adult can have a bigger effect in a child, including:
- Inflammation or swelling (edema)
- Thick mucus
- Blood or vomit
- A foreign object
When the airway is narrow, there’s simply less room for air to move through.
This is why:
- Respiratory illnesses can sound intense in kids
- Small changes can create big symptoms
- Early support (humidity, saline, positioning) can make a noticeable difference
It also explains why noisy or labored breathing gets attention quickly in pediatric care — not because every case is dangerous, but because children have less margin for obstruction.
2. Infants Are Preferential Nose Breathers
Infants — especially those under 6 months of age — primarily breathe through their noses.
This means:
- Even mild nasal congestion can significantly impact breathing
- A stuffy nose can cause feeding difficulty, poor sleep, and respiratory distress
- Nasal support (saline, suctioning, humidification) is often more important than parents realize
For young infants, clearing the nose can dramatically improve breathing.
3. Children Have Higher Metabolic Rates and Faster Breathing
Infants and children naturally breathe faster than adults because they have:
- Higher metabolic demands
- Greater oxygen needs relative to body size
When illness or injury occurs, the metabolic rate increases further. This leads to:
- Increased respiratory rate
- Greater insensible fluid loss (fluid lost through breathing and skin)
- Higher risk of dehydration, which can worsen respiratory symptoms
This is why hydration is a core respiratory support, not an afterthought.
4. Lower Oxygen Reserves Mean Faster Desaturation (Drop in Oxygen)
Children also have:
- Smaller oxygen reserves
- Less ability to tolerate prolonged stress on the respiratory system
Because of this, oxygen levels can drop more quickly during illness.
To compensate, the body responds by:
- Increasing breathing rate
- Increasing work of breathing
This compensation takes a lot of energy.
5. Fatigue Can Signal Decompensation
At first, children often compensate well.
But after prolonged effort:
- Energy reserves become depleted
- Muscles fatigue
- Breathing may become less effective
This is why fatigue, lethargy, or a sudden decrease in effort can actually be more concerning than noisy breathing alone.
This is why monitoring matters — a child who suddenly becomes quiet, stops fighting, or appears exhausted may be tiring out and losing the ability to compensate, even if they were previously working hard to breathe. If you see this change, seek immediate medical evaluation.
6. Abdominal Breathing Is Normal — Until It’s Not
Abdominal (belly) breathing is common and normal in:
- Infants
- Young children under about 7 years old, whose chest muscles are still developing
They rely more heavily on the diaphragm to breathe.
However:
- Abdominal breathing becomes more pronounced during respiratory distress
- Excessive belly movement, paired with retractions or rapid breathing, can indicate increased work of breathing
Context matters — belly breathing alone isn’t a red flag, but changes from baseline are important.
7. A Note on Periodic Breathing and Apnea (Pause in Breathing) in Infants
In preterm infants:
- Periodic breathing (brief pauses up to ~10 seconds) can be normal
Apnea is defined as:
- Cessation of breathing for 20 seconds or longer, or
- Shorter pauses accompanied by color change, limpness, or bradycardia (heart rate dropping significantly below normal age — in infants, a heart rate below 60bpm is a medical emergency).
This distinction is important to avoid unnecessary panic — while still recognizing true emergencies.
8. Why Swelling Matters More Than Mucus
Parents are often taught to worry most about mucus. In reality, mucus is protective. It traps pathogens and helps move them out of the body.
What causes the most distress in respiratory illness is inflammation and swelling, not mucus itself.
When the airway swells:
- Air has less room to move
- Breathing becomes noisy
- Coughs can sound barky, harsh, or alarming
This is why illnesses like croup, viral laryngitis, and post-viral coughs can sound intense — even when the body is doing exactly what it’s supposed to do. We’ll go over supports for all this below.
Why Respiratory Symptoms Worsen at Night
Parents often notice that their child’s breathing issues seem manageable during the day, only to suddenly intensify at night.
This isn’t random — there are physiological reasons behind it.
Circadian Rhythm and Inflammation
At night, cortisol levels naturally drop. Cortisol is anti-inflammatory, so when it dips, inflammation increases.
That means:
- Increased airway swelling
- Louder and more labored breathing
- More frequent coughing
Lying Flat and Airway Narrowing
When children lie down:
- Gravity changes how secretions (mucus) drain
- The airway naturally narrows
- Congestion and inflammation often feel worse
This is why many respiratory flare-ups begin suddenly just after bedtime.
What This Means for Parents
Nighttime worsening does not automatically mean danger. It is often a predictable part of the body’s rhythm.
It does mean:
- Extra support may be needed at night
- Positioning, humidity, and calming strategies play a bigger role
- Close monitoring is important
Understanding this normal pattern can reduce a lot of anxiety and help parents respond calmly and effectively.
Foundations of Respiratory Health (Before Illness)
The best time to support respiratory health is before symptoms even appear.
Humidity Is Non-Negotiable
Indoor humidity plays a massive role in respiratory health.
Ideal range: 40–60% you can easily check this with a hygrometer – a humidity reader (find one HERE)
Humidity helps:
- Keep mucus thin
- Support cilia movement (tiny airway cleaners)
- Reduce airway irritation
Cool-mist humidifiers are my preference and are generally safest for families (this is the one I use). Warm mist can be helpful short-term but poses burn risks for young children.
Nasal Breathing and Airway Prep
The nose is our body’s first line of defense — it warms, filters, and humidifies the air.
Support clear nasal breathing with:
- Saline sprays or nasal sprays
- Gentle nasal hygiene
- Gentle nasal suctioning (I use this battery-powered one)
Good nasal care can significantly reduce lower airway irritation during illness and help kids breathe easier when sick.
Hydration and Electrolytes
Hydration directly affects mucus thickness. Thin secretions are easier to clear, while dehydration thickens mucus and worsens coughing.
Offering small, frequent sips is often better than large amounts — especially when kids aren’t feeling well and appetite or energy is low.
Our family uses these electrolytes (grape is our favorite, Code: VITALITYASH) or we use coconut water for natural electrolyte support.
Hydration helps maintain:
- Better overall comfort and energy
- Thinner secretions (mucus)
- Easier coughing (can effectively clear)
- Prevents dehydration
Immune Support
A strong baseline immune system can shorten illness and reduce symptom severity. We focus on sustainable, daily habits — not quick fixes.
Key pillars we focus on:
- Nutrition: adequate protein, minerals, and healthy fats to support immune function
- Vitamin D & K2: supports immune signaling and respiratory defense, especially in fall and winter
- Vitamin C: supports immune cells and tissue repair during illness
- Zinc: plays a key role in antiviral defense and mucosal (airway) immunity
- Gut health: much of the immune system lives in the gut
- Sleep + nervous system regulation: rest and regulation directly impact immune response
These supports don’t replace medical care — they simply help the body respond more effectively when illness hits.
Early Respiratory Support (When Symptoms First Start)
How you respond in the first 24 hours often shapes how the rest of the illness unfolds.
What I Watch First (Behavior Over Sounds)
Before I focus on the cough itself, I look at:
- Energy level
- Skin color
- Ability to drink fluids
- Overall comfort vs distress
A noisy child who is drinking, responsive, and calms with support is very different from a child who looks pale, exhausted, or persistently distressed. Behavior tells me far more about how sick a child is than sounds alone.
Supporting Active Respiratory Illness at Home
Nebulized Saline
Nebulized saline delivers moisture directly to the airways. We use this 0.9% saline and this handheld nebulizer or this plug-in nebulizer.
Benefits include:
- Soothing airway irritation
- Thinning secretions
- Making breathing more comfortable
Saline is supportive, not suppressive, and is well tolerated. It is generally safe for all ages.
Note: 3% saline (hypertonic saline) can help thin thicker mucus, especially in infants with conditions such as bronchiolitis or RSV. It should be used under clinical guidance for very young children or those with complex respiratory needs.
Steam Therapy
Steam can be helpful for soothing upper airway irritation (think Croup-like, barking coughs).
To use steam safely:
- Sit with your child in a steamy bathroom for 10–15 minutes.
- Close the door, run the shower on the hottest setting, and let steam fill the room.
- Do not place your child directly in hot water.
Warm, moist air reduces tissue swelling and helps loosen mucus, but not every child responds the same. Some find steam comforting, while others may prefer cooler air.
Cool or Cold Air
Cool air can reduce airway swelling and is especially helpful for barky coughs, stridor, or croup-like symptoms.
Simple options:
- Step outside briefly into cool air (bundle child up)
- Open a window and stand by it
- Stand in front of an open freezer if it is not cool enough in your region
This can provide surprisingly fast relief.
A powerful combination: steam therapy followed by exposure to cool air often lessens swelling in the upper airway, making breathing easier and calming coughing fits.
Positioning and Gentle Movement
Keeping children upright can:
- Improve airflow
- Reduce pooling of secretions
- Make breathing feel easier/more comfortable
Upright rest (prop up with pillows), cuddling in a chair, or gentle rocking can help. Balance movement with periods of rest; both matter.
Rest, Regulation, and the Nervous System
Breathing difficulty can feel scary — for both you and your child.
Creating a calm environments helps regulate:
- Breathing patterns
- Heart rate
- Nervous system response
Your calm, reassuring presence often provides more comfort than any other intervention.
Chest Percussion
Chest percussion is a gentle technique that helps loosen mucus so it’s easier to cough up.
To try it:
- Use light, rhythmic tapping with a cupped hand on the upper and mid-back or sides of the chest (avoid the spine and neck).
- Perform for 2–5 minutes, then pause.
- It’s most effective after humidity, steam, or saline treatments have already softened secretions.
Chest percussion is best suited for wet, congested coughs, not for dry, barky coughs caused mainly by airway swelling.
You can watch a visual demonstration here.
Natural Supports for Respiratory Comfort
These are supportive tools and are best used as part of a bigger picture.
Topical Supports
- Chest rubs/salves
- like Earthley’s Breathe Well Salve HERE (code ASHLEYG), or Badger’s HERE can offer gentle comfort on the chest, back, or soles of feet. Avoid conventional menthol/camphor rubs in children under 2, as they can irritate baby airways.
- Socks
- Onion socks
- Garlic socks (use a barrier to protect the skin)
- Cold Wet Socks Remedy (supplies here)
- Compresses On the Chest
- Salt Compress
- Mustard Seed Poultice (do not use on children under 3 years or anyone asleep, watch closely for skin irritation and remove immediately if redness or burning occurs)
- Castor oil packs (never on broken skin; avoid over the chest in very young children)
- Baths
- Magnesium flakes or Epsom salt baths
- Essential Oil in baths
- Only a few drops, well-diluted, and use kid-safe options for young children
- Thyme Essential Oil in bath (just a few drops)
Oral Supports
- Whole-food vitamin C
- High dose Vitamin C Protocol
- Herbal teas for throat and airway comfort, as an expectorant, for immune support, for fever support,
- Flu tea
- Little lungs tea (Michelle-is-Well code ASHLEY)
- Thyme tea
- Fennel-hyssop tea
- Mullein-sage tea
- Peppermint tea with sage and comfrey
- Holy basil tea
- Rosemary tea
- Sage-lemon tea
- Elderflower tea
- Chamomile tea
- Ginger tea
- Lemon balm tea
- Respiratory Tonic
- Herbal tinctures
- Earthley’s cough-be-gone (Code ASHLEYG)
- Echinacea (with or without goldenseal)
- Ashwaghanda
- Astralgus
- Grapefruit Seed Extract
- Thyme
- Herbal syrups
- Elderberry Syrup
- Cold Syrup with comfrey, mullein, and raspberry leaf
- Licorice-Thyme Cough Syrup
- Thyme and Cherry Bark Cough Syrup
- Cold & Flu Syrup
- Cough and Lung Syrup
- Loquat Syrup
- Honey to soothe throat and cough
- Local raw honey or Manuka Honey is best (not recommended for children under 1 year of age due to botulism risk)
- Honey Infusions
- Fermented Garlic Honey
- Onion Honey
- Rosemary Honey
- Oxymels (herbs infused in a honey + vinegar base)
- Thyme oxymel
- Fluids and broths
- Bone broth for electrolytes and nutrients
- Electrolytes from Just Ingredients (code VITALITYASH)
- Coconut water
- Kudzu-Apple Juice
- Garlic lemonade
- Lozenges
- Beekeepers Naturals (they have lozenges and lollipops – choose age appropriate options to avoid choking)
- Slippery Elm
*Note: licorice, comfrey, sage, and thyme may be contraindicated in certain conditions such as pregnancy, hypertension, liver disease etc. Always check with a trusted healthcare provider before starting any herbal supplements.
Inhalation
- Herbal steams
- peppermint, thyme, chamomile, etc
- Essential oil diffuser (using kid safe oils and proper dilution)
- Onion or onion honey in bowl by the bed as a gentle, traditional support
Homeopathy
Some families choose homeopathy for individualized support. This approach is highly specific and works best when tailored to the child and symptom picture. Here are some common ones and their indication:
- Oscillococcinum (Oscillo) — flu-like symptoms with body aches, chills, and fatigue
- Cold Calm / Cold Calm Baby – combo remedy used for cold symptoms, cough, and mucus.
- Chestal / Chestal Honey – combo remedy for cough and mucus relief, nasal or chest congestion, and sore throat relief
- Aconite – Sudden onset of symptoms, often after cold wind exposure; anxiety, restlessness, early fever, dry cough
- Belladonna – Rapid onset with heat, redness, throbbing, inflammation; hot face, fever, sensitivity, sudden worsening
- Spongia tosta – Dry, barking, croup-like cough; hoarseness; cough sounds like a saw through wood, often worse at night
- Hepar sulphuris – Loose, rattling cough with thick mucus; very sensitive to cold air; irritability
- Drosera – Deep, spasmodic coughing fits; worse at night or when lying down; coughing until gagging or vomiting
- Antimonium tartaricum – Chest congestion with difficulty clearing mucus; rattling sounds but weak cough
- Phosphorus – Tight chest, cough worsened by talking or laughing; thirst for cold drinks; fatigue
- Sambucus nigra – Nighttime respiratory distress, nasal congestion, sudden waking with difficulty breathing
- Pertussinum — spasmodic, repetitive coughing fits, especially when coughing comes in waves
Red Flags vs What is Normal During Healing
Normal During Healing
What Can Look Scary but Be Okay
- Barky or harsh coughs that improve with support (positioning, humidity, cool air)
- Noisy breathing that settles with rest, positioning or humidity
- Lingering cough after other illness symptoms resolve (a “tail” cough that slowly fades)
Healing is rarely linear – good stretches and tough patches can alternate.
Signs Things Are Improving
- Longer stretches of comfortable sleep
- Improved hydration and more frequent wet diapers/urine
- Easier breathing between coughing episodes
- More normal play/interaction
Red Flags: When I Would Seek Medical Care
Most respiratory illnesses can be supported at home — but there are times when medical care is absolutely the right choice.
As an ER nurse, these are the specific things I watch for in my children, regardless of the diagnosis.
I don’t make the decision to go to the ER based on one sign alone.
Breathing concerns are nuanced, and multiple things are often happening at once.
That said, I seek emergency care when breathing concerns are paired with red flags.
Signs of Increased Work of Breathing
These indicate your child is working harder than they should to breathe:
- Retractions (skin pulling in with breaths)
- The higher the retractions go, the harder the child is working
- Subcostal (below ribs: mild-moderate) →
- Intercostal (between ribs: moderate) →
- Substernal (below breastbone: moderate-severe) →
- Suprasternal (tracheal tug – at the neck: severe) →
- Supraclavicular (above collarbones: most severe)
- Grunting with breaths
- Head bobbing (especially in infants)
- Nasal flaring (particularly if paired with color or behavior changes/red flags)
- Rapid breathing that does not slow with rest, comfort, or being held
Behavior and Energy Red Flags
These are often more important than the sounds you hear:
- Lethargy or extreme fatigue
- Floppiness or poor muscle tone
- Difficulty waking or staying awake
- A child who suddenly becomes quiet after working hard to breathe
- Weak cry or inability to speak or cry normally
A child who is tiring may actually look less dramatic — but this can signal decompensation (worsening condition).
Oxygen and Circulation Red Flags
These require urgent evaluation:
- Blue or gray color around the lips or mouth (cyanosis)
- Blue nail beds
- Mottling of the skin (patchy color)
- Slow capillary refill (pressing a finger or toe and color takes >2 seconds to return to pink)
- Pale, ashen, or “washed out” appearance
These signs suggest oxygenation or circulation may be compromised. I would consider calling an ambulance for these concerns while also continuing other supportive measures. As I previously stated, there are often multiple things happening at once.
Breathing Pattern Red Flags
- Pauses in breathing (apnea) — especially in infants (where they stop breathing for longer than 20 seconds)
- Stridor at rest (high-pitched breathing noise when not crying or upset that does not improve with steam and cool air OR if you suspect a foreign body) often accompanied by suprasternal retractions
- Any sudden change from a stable pattern to very labored, noisy, or silent breathing
Feeding and Hydration Concerns
Especially important in infants and young children:
- Inability or refusal to drink or feed
- Falling asleep during feeds due to fatigue or breathing effort
- Signs of dehydration (dry mouth, minimal urine output, no tears when crying, sunken fontanelles for infants)
- Vomiting with coughing that prevents them from keeping all fluids down
Monitoring and Intuition
- Oxygen saturation below about 92% (if you have a pulse oximeter monitor that you know how to use and trust) can be a concerning sign when paired with clinical red flags (one with wavelength detection here, budget option here).
- My gut instinct — if something feels off, I listen to it
It’s rarely one symptom. It’s the combination that matters.
Bottom Line : Trust Your Intuition
If your child looks or feels off to you — even if you can’t name why — go in.
You are not overreacting. You know your child best, and seeking help early is part of good, attentive parenting.
What to Expect If You Go to the Emergency Room
Initial Assessment
When you arrive at the ER, you’ll first check in and be triaged by a nurse.
The second the triage nurse lays eyes on your child, they will be conducting what is called an across-the-room assessment.
In pediatric care, this is formally known as the Pediatric Assessment Triangle (PAT) — a rapid, visual assessment used to determine how sick a child is before any equipment is placed or vital signs are taken.
The nurse is immediately assessing three things:
1. Appearance
How your child looks and behaves:
- Are they alert or lethargic?
- Do they have good muscle tone or do they appear floppy?
- Are they interacting appropriately for their age?
- Is their cry strong, weak, or absent?
Appearance is often the most important indicator of how well a child is compensating.
2. Work of Breathing
How hard your child is working to breathe:
- Retractions (are they present and how high are they?)
- Nasal flaring
- Grunting
- Head bobbing
- Abnormal breathing patterns
- Audible sounds like stridor or wheezing
This helps identify respiratory distress even before oxygen levels are measured.
3. Circulation to the Skin
How well oxygenated and perfused your child appears:
- Skin color (pink, pale, mottled, blue, or gray)
- Color around the lips and mouth
- Overall perfusion
Changes here can signal compromised oxygenation or circulation.
This assessment happens within seconds and guides how urgently your child needs to be seen.
If the PAT is concerning, your child may bypass the waiting room and be taken straight back to a treatment room to be evaluated immediately.
They will then be triaged.
Triage
During triage, the nurse will:
- Take vital signs, including:
- Oxygen saturation
- Respiratory rate (counted for a full minute)
- Heart rate
- Temperature (often rectally if under the age of 2)
- Blood Pressure (age dependent)
- Ask about:
- What symptoms you have noticed
- When symptoms started
- How they’ve changed
- Feeding, hydration, and behavior
- What you’ve already tried at home
- Your child’s medical history. Including: allergies, past medical conditions, surgeries, medication history, vaccination status etc.
Your child will be assigned an acuity level, which determines how quickly they are seen.
If immediate care is needed, a provider will evaluate them right away.
Evaluation and Supportive Care
Once in a room, a provider will assess your child.
Depending on the situation, treatment may include:
- Nebulized medications (like epinephrine to reduce airway swelling)
- Steroids
- Often given orally (like dexamethasone or prednisolone)
- IV steroids may be used if a child is very sick
- Oxygen support
- Blow-by oxygen
- Humidified oxygen
- High-flow oxygen in some cases
For many pediatric respiratory illnesses, ER care is largely supportive — helping the child breathe more comfortably while the body recovers.
Observation, Reassessment, and Disposition
After treatment:
- Your child will be observed in the ER (they want to ensure that there is no rebound respiratory distress after the medications wear off)
- Vital signs and breathing effort will be reassessed periodically
- Providers will monitor for clear improvement or worsening symptoms/signs more support is needed
If your child improves and remains stable, they are often discharged with home‑care instructions and clear return precautions.
If symptoms remain concerning, admission to the hospital may be recommended.
Reassurance and Final Thoughts
Going to the ER does not mean you failed at home care.
It means you recognized when more help was needed.
Support at home → escalation when appropriate.
Respiratory illness is one of the most common — and most stressful — parts of parenting.
Understanding how children’s airways work, why symptoms can escalate quickly, and how to support the body at home can replace panic with preparedness. Most of the time, supportive care is enough. Sometimes, medical care is needed — and recognizing that moment is part of good parenting, not a failure.
There is no prize for waiting too long and no shame in going in early.
The goal isn’t to avoid the ER at all costs — it’s to care for your child wisely and confidently.
With a well-supported home, a calm approach, and clear red flags in mind, parents are better equipped to navigate respiratory illness with steadiness instead of fear.
You’ve got this. You’re doing an incredible job showing up, learning, and advocating for your child’s health.
If you found this helpful, I’d love to connect with you over on Instagram. I share ongoing education, natural remedies, real-life parenting, and practical tools for low-tox living – and living a life of vitality @vitalityash.





2 Comments